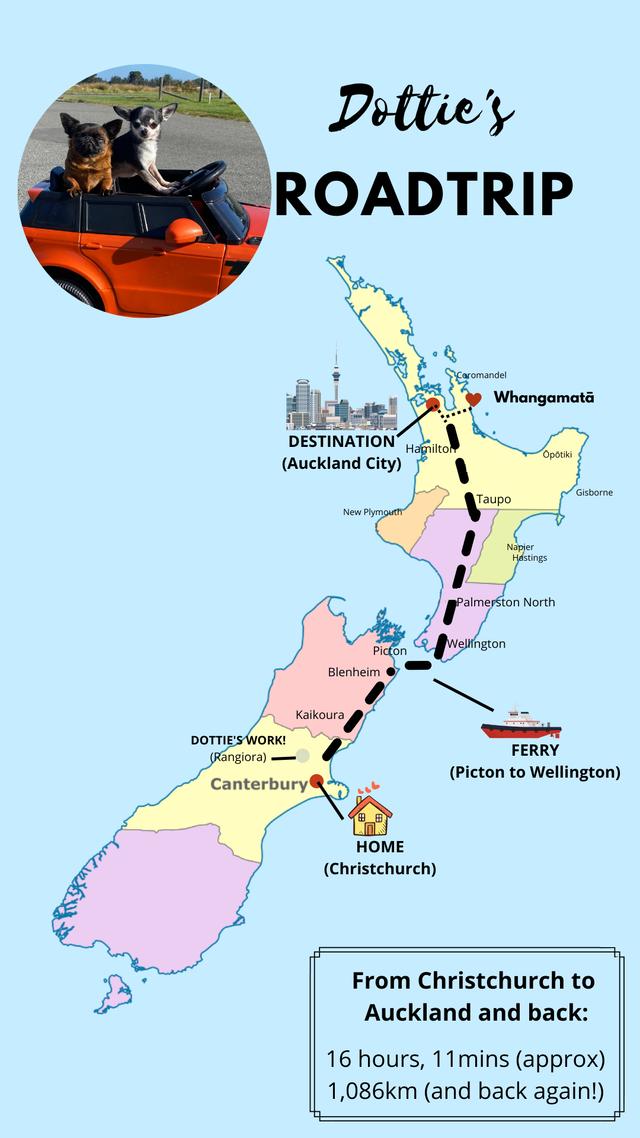
On Tuesday 18th May 2022 about 4am after 16+ hours travelling by car and ferry, we made it to Auckland!
As most of you know, for the past month our focus has been on getting Dottie to Auckland for a MRI with a Neurologist present. I’ve summarised the reasons why we needed to leave Christchurch in a prior blog. A more precise MRI is required so we can understand what Dottie’s brain looks like and what’s going on with regards to her pain and neurological health.
Originally, Dottie was supposed to have a spinal tap completed at the same time. But the Neurologist didn’t feel that this was required as: 1) Dottie has no evidence of inflammation on her MRI; 2) This would be to rule out Meningitis. But Dottie improved after she was taken off prednisone (steroids) and if she had this, she would have deteriorated; 3) The MRI took a bit longer than anticipated and they felt Dottie had been anesthetised for long enough.
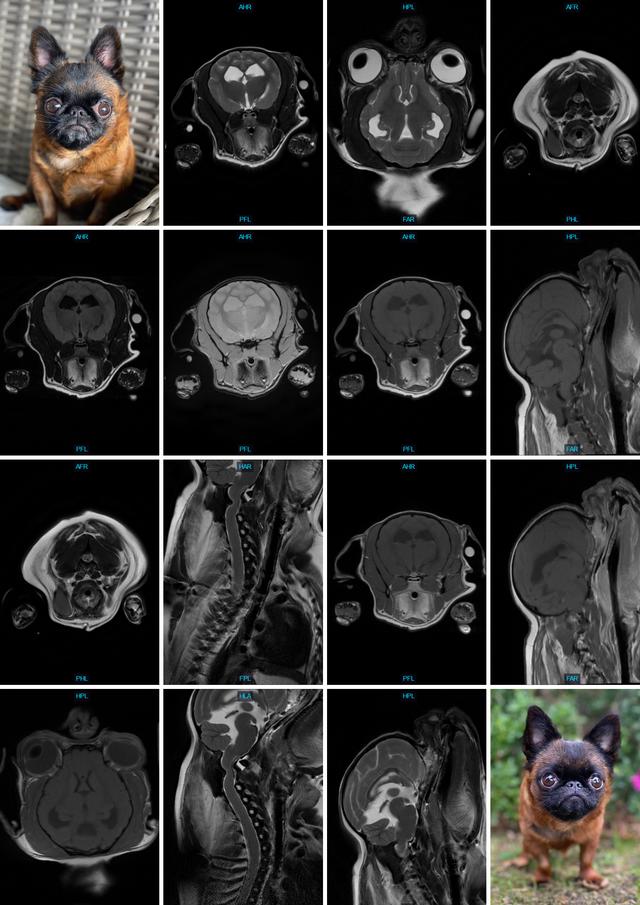
The following day, we went back to the clinic to have the IV removed. We also got to look at Dottie’s MRI images and discuss the findings with her Neurologist, Dr Georgina Stewart.
Although it was a bit of trouble getting Dottie to Auckland, with the ups and downs of transport laws, the standard of care and investigation into her health was DEFINITELY worth it! I encourage every pet owner to go in search of the best care for their animals.
We already knew Dottie has Chiari like malformation (CM) which progresses to Syringomyelia in most cases (SM). With the seizure episodes she had on 31st March 2022, we became worried that this was the case with Dottie.
In addition to that, the 15th June 2021 MRI seemed to show some sort of compression issue with her spinal cord. The Doctors were concerned Dottie had a serious neck instability.
MRI Findings
The results of the MRI showed a couple of things.
1. We can be fairly confident from the MRI that the Chiari-like malformation has not progressed to syringomelia at the moment (ie. this is amazing news!!).
2. They are fairly sure her neck is okay, impossible to tell without cutting and looking at it for sure. But surely, if it were terrible, it would have shown more clearly on the MRI (ie. so we think that this is fairly good news too!)
From the MRI Report: “A flexed lateral view of the cervical spine is provided and there is no evidence of improvement of the spinal cord compression in the craniocervical region or instability at the atlantooccipital or atlantoaxial junction.”
3. Her ventricles (the fluid filled sacs in the brain) are enlarged, also known as a quadrigeminal cyst. This is compressing the other structures of her brain. It can lead to pressure in the brain causing pain, nausea, a and seizures. (Shit news but not dreadful)
From the Report: “The patient has a symmetrical mild ventriculomegaly of the lateral ventricles. No periventricular edema is identified. The third ventricle is also dilated and the interthalamic adhesion is oblong in contour suggestive of increased intracranial pressure. The fourth ventricle is dilated to a moderate degree. There is a moderate sized cystic dilation within the quadrigeminal cistern. This is causing caudal displacement and flattening of the cranial margin of the cerebellum. No signs of occipital dysplasia are noted. No signs of cerebellar herniation are noted although the contour of the caudal aspect of the cerebellum is abnormal.”
4. Dottie has a deviated septum! (An incidental finding)
From the Report: “Nasal septal deviation is noted as an incidental finding. There is increased intensity of the paravertebral musculature of the cervical spine compatible with chronic fatty atrophy. The soft tissues of the skull and cervical region are within normal limits otherwise. No lymphadenopathy is evident.”
5. Dottie’s main finding was that she has an abnormal growth (“dorsal compressive lesions at the antlantoaxial band” or “junction” the fancy term) in her skull. This is what has produced the “kink” in her spinal cord image.
From the Report: “Dorsally at the atlantoaxial junction there is a prominent bony protuberance extending ventrally into the vertebral canal causing marked compression of the cranial cervical spine at this point. The C1 lamina is concave and this contour is causing this ventral deviation of the caudal aspect of the C1 lamina. The combination of changes in the cranial cervical spinal cord causes a sigmoid flexure at this site.”
This dorsal compressive lesion is basically a growth pressing into her spinal cord or compressing it, which will be the cause of her pain. It could be made out of bone or scar tissue, they need to open her up and look at it to determine. They don’t know whether she was born with it, or if it grew there.
This cord compression will cause pain, but is also likely the reason she presses her head. Also, when she looks up, she is unable to lift up her head and has to tilt sideways, with her little leg lifted. Lifting her head or holding it up throughout the day will put pressure on that juncture, causing pain. This could be why she is more alert and bright in the mornings.
Dottie may be able to manage the pain associated with this compression with pain medication. But it will not get better unless it is removed surgically. There are pro’s and cons to leaving it or operating.
Pros:
- If we do not operate, she will continue being in pain sometimes. If we operate, it could remove this pain completely!
- If we choose to operate, Dottie will hopefully retain her mobility. If we left it as is, she may end up losing her mobility or left paralysed. At best, it remains as it is, but she’ll need regular MRI’s and monitoring.
Cons of Operating:
- Surgery may correct the issue. Especially if it is bone, as then it likely will not re-grow. If it is scar tissue or some other growth, we may go through the trouble to remove it just to have it come back.
- In addition to this, the growth is very close to her nerves which control the respiratory system and one mistake could mean immediate death for Dottie. It is a very risky surgery.
- The doctors also have to cut through her muscles in the back of her neck too, so the recovery is very long and tough. Dottie won’t be able to lift her head (as those muscles allow her to do that) and remain at the vets for 5-7 days. It will be such a tough recovery on her!
I can’t help but think that if we were brave to take the risk and help Dottie through her recovery, it could change her whole life. Dottie will always live with a bit of pain due to her joint and bone issues, true. But this is something we could help her with and possibly take away her pain. We could really improve her quality of life. For that reason, we do need to research it and think on it carefully. We really want Dottie to be comfortable enough to be around for many, many years to come!
What Happens Next?
At the moment, we are continuing her on her pain medications (Gabapentin) and Omeprezole (for the brain fluid).
We have a consult booked for 26th May 2022 (at 11.30PM NZT and 7.30AM Miami time) with Dottie’s USA-based Neurologist, Dr DePompa. We want to hear his recommendations and analysis of the MRI results also. New Zealand tends to be fairly conservative when it comes to surgical treatments and we know DePompa has a lot of experience with neuro cases.
I have to admit, a lot of relief came with this scan in a couple of ways, although it’s not 100% great news. At the moment, we are just trying to recover from the long trip and look at the positives. Dottie’s neck is OK, no SM so far and nothing immediately terminal. We will research more, think on what is best for Dottie and try to decide either way.
Thank you to everyone who has donated, shared the Givealittle link and sent your lovely well wishes to Dottie so far. Your support has been a huge source of strength to us in the dark times we’ve been through recently. Little Miss Dottie Walters, her mum, dad and other fur siblings are eternally grateful for all of your support.
Although Dottie has a little bit of work ahead of her, we know she has the very best care possible and her pain is managed. Dottie is not suffering unnecessarily and still has a good quality of life. If she didn’t, there is no way we would ask her to continue. But Dottie enjoys her life, she is bright, happy, clever and very loving. It bothers us to see comments about euthanasia as if her life is not worth fighting for. You clearly don’t know Dottie if you think that is her best option. Dottie still deserves a chance and that is what we will give her.
As always, we will keep you updated.
Report Information (Additional Info and Big Words!!):
Neurolocalisation: Normal neurological function with reduced cervical range of motion.
Differential Diagnoses:
1. Chiari-like malformation +/- syringomyelia
2. Atlanto-axial subluxation +/- dorsal band
3. Meningoencephalitis (immune mediated)
Dottie presented to ARC Neurology Service for evaluation of her neurological function and a repeat MRI. On examination Dottie was very bright and happy with excellent ambulation. Her gait was somewhat impaired due to her orthopedic conditions but she had no evidence of ataxia. Her neurological function was normal but she was found to have slightly reduced range of motion of her head and neck and a tendency to pick up one front leg while looking around.
Dottie underwent an MRI scan of her brain and cervical spine which showed several abnormalities. The most significant changes are associated with the back of her skull and the first 2 vertebrae in her neck - she has a mild Chiari-like malformation and a dorsal spinal cord compression at the level of the C1-2 junction referred to as a dorsal band or AA band. She does not have any evidence of syringomyelia or atlanto-axial luxation. She has an accumulation of fluid in the back part of the brain causing compression of the cerebellum referred to as a quadrigeminal cyst or supracollicular fluid accumulation. A spinal fluid sample was not obtained due to no evidence of inflammatory brain/spinal cord disease on the scan
The next steps for Dottie involve altering her pain management protocol and deciding if surgical decompression of her dorsal band should be pursued. It is impossible to say if her dorsal band will progress or remain static. Surgery is fairly straightforward but does come with the risk of complications such as neurological worsening or even death. Dottie's MRI and clinical findings today will be shared with her care team and a long term plan put together for her!
PROCEDURE/RESULTS:
1. MRI (brain/cervical spine): Cranial cervical vertebral malformation of the caudal aspect of C1 and dorsal C1-2 junction causing severe spinal cord compression. No instability of the atlantoaxial joint is noted. No syringomyelia is present. A large supracollicular accumulation of fluid is present (quadrigeminal cyst) causing mild compression of surrounding structures.
CONCLUSIONS:
The patient has multiple congenital anomalies with the primary abnormality being a cranial cervical vertebral malformation at the atlantoaxial junction leading to dorsal spinal cord compression due to the abnormal conformation of the C1 lamina and potentially C1-C2 dorsal articulation. There is also elevation of the brainstem at the atlantoaxial junction although this is potentially within normal limits. This intense, severe spinal cord compression at C1- C2 is the likely source of clinical signs. No signs of syrinx formation are noted in
association.
The patient has evidence of increased intracranial pressure although this may be limited to the quadrigeminal cistern and third ventricle given that the cerebral mantle has normal sulci visualized which would typically not be present if there were increased intracranial pressure. This may be associated with a chronic congenital abnormality causing differential pressure in different portions of the calvarium and potentially cerebral atrophy of a degree. The patient does have a quadrigeminal intraarachnoid cyst that is moderate in size that is compressing this cerebellum. The significance of this cyst is uncertain.